
Head injuries in children can very easily fall into the grey area, where you're not sure whether the child needs a CT or not, and sometimes they fit the guidelines, but really don't need a CT... Page 9 of the NICE guidelines is very clear about when people need a CT, and there's a nice crib sheet from @_NMay here.
The most debated point on the NICE guidelines seems to be "three or more discrete episodes of vomiting". The BMJ has investigated vomiting, and found it to be an unreliable sign. The SIGN guidelines report "repeated vomiting is a weaker predictor (RR 0.88) with reported OR ranging from 2.13 to 4.08 in three studies. In children, repeated vomiting had a PPv of 0.065". Yet they still suggest scanning these children. There's even a best bet saying vomiting isn't an accurate predictor although there is another best bet suggesting that persistent vomiting warrants a scan.
Children do vomit after an injury. If they don't get pain killers quickly enough, they vomit some more. They're prone to gastroenteritis and other bugs that make them vomit. And we don't like irradiating children because of the radiation risk. Trouble is, we're often happy to watch and wait, parents are often happy to watch and wait, but the admitting paediatric team (paediatricians, paediatric surgeons, neurosurgeons - who ever they come in under in your hospital) often want the reassurance of a normal CT scan before they'll admit. As Emergency Literature of Note notes, observation is often safer than a CT.
There are podcasts out there (and here and here) about head injuries.
There is another rule out there that is a lot more simple and doesn't include vomiting as a criteria - CATCH. Then there's CHALICE and the Kuppermann head CT rules, aka PECARN (summarised here, with a link to the original article and another podcast here). These three rules are compared by the EMJ here, and online here. Importantly CHALICE and CATCH identify those who need a CT, and PECARN identifies those who do not:
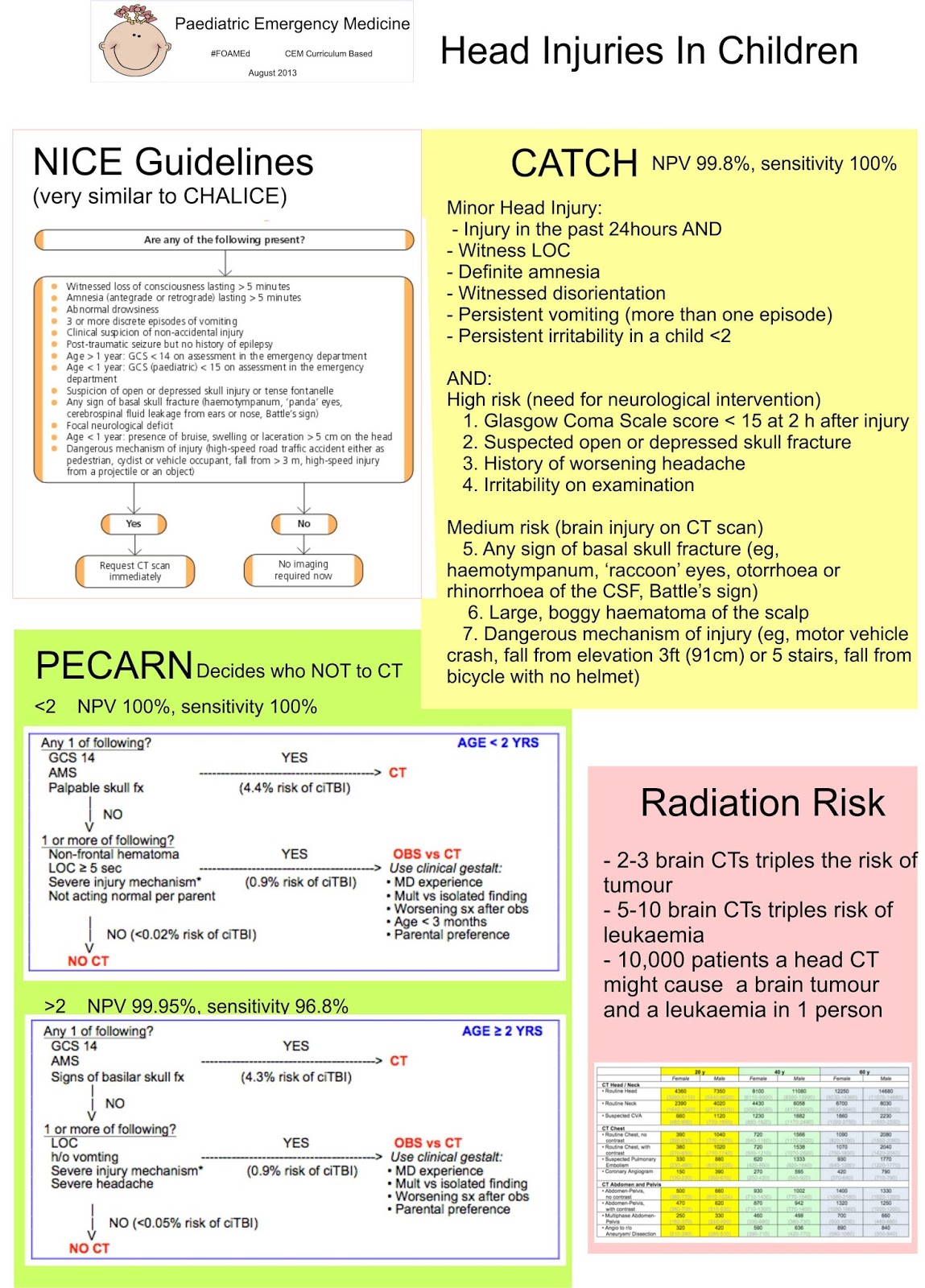
PECARN
<2 NPV 100%, sensitivity 100%
>2 NPV 99.95%, sensitivity 96.8%
CHALICE
NPV 99.9%, sensitivity 98%
CATCH
NPV 99.8%, sensitivity 100%
<2 NPV 100%, sensitivity 100%
>2 NPV 99.95%, sensitivity 96.8%
CHALICE
NPV 99.9%, sensitivity 98%
CATCH
NPV 99.8%, sensitivity 100%
CATCH Rule (Canadian Assessment of Tomography for Children with Head Injury):
CT of the head is required only for children with minor head injury* and any one of the following findings:
High risk (need for neurological intervention)
1. Glasgow Coma Scale score < 15 at 2 h after injury
2. Suspected open or depressed skull fracture
3. History of worsening headache
4. Irritability on examination
Medium risk (brain injury on CT scan)
5. Any sign of basal skull fracture (eg, haemotympanum, ‘raccoon’ eyes, otorrhoea or rhinorrhoea of the CSF, Battle’s sign)
6. Large, boggy haematoma of the scalp
7. Dangerous mechanism of injury (eg, motor vehicle crash, fall from elevation 3ft(91 cm) or 5 stairs, fall from bicycle with no helmet)
*Minor head injury is defined as injury within the past 24 h associated with witnessed loss of consciousness, definite amnesia, witnessed disorientation, persistent vomiting (more than one episode) or persistent irritability (in a child <2 years of age) in a patient with a Glasgow Coma Scale score of 13/15.
CHALICE Rule (Children's Head Injury Algorithm for the Prediction of Important Clinical Events):
A CT scan is required if any of the following criteria are present.
High risk (need for neurological intervention)
1. Glasgow Coma Scale score < 15 at 2 h after injury
2. Suspected open or depressed skull fracture
3. History of worsening headache
4. Irritability on examination
Medium risk (brain injury on CT scan)
5. Any sign of basal skull fracture (eg, haemotympanum, ‘raccoon’ eyes, otorrhoea or rhinorrhoea of the CSF, Battle’s sign)
6. Large, boggy haematoma of the scalp
7. Dangerous mechanism of injury (eg, motor vehicle crash, fall from elevation 3ft(91 cm) or 5 stairs, fall from bicycle with no helmet)
*Minor head injury is defined as injury within the past 24 h associated with witnessed loss of consciousness, definite amnesia, witnessed disorientation, persistent vomiting (more than one episode) or persistent irritability (in a child <2 years of age) in a patient with a Glasgow Coma Scale score of 13/15.
CHALICE Rule (Children's Head Injury Algorithm for the Prediction of Important Clinical Events):
A CT scan is required if any of the following criteria are present.
- History
- Witnessed loss of consciousness of >5 min duration
- History of amnesia (either antegrade or retrograde) of > 5 min duration
- Abnormal drowsiness (defined as drowsiness in excess of that expected by the examining doctor)
- > 3 vomits after head injury (a vomit is defined as a single discrete episode of vomiting)
- Suspicion of non-accidental injury (NAI, defined as any suspicion of NAI by the examining doctor)
- Seizure after head injury in a patient who has no history of epilepsy
- Examination
- Glasgow Coma Score (GCS) <14, or GCS <15 if < 1yearold
- Suspicion of penetrating or depressed skull injury or tense fontanelle
- Sign of a basal skull fracture (defined as evidence of blood or CSF from ear or nose, panda eyes, Battle’s sign, haemotympanum, facial crepitus or serious facial injury)
- Positive focal neurology (defined as any focal neurology, including motor, sensory, coordination or reflex abnormality)
- Presence of bruise, swelling or laceration >5cm if < 1 year old
- Mechanism
- High speed road traffic accident either as pedestrian, cyclist or occupant (defined as accident with speed > 40 m/h)
- Fall of > 3 m in height
- High speed injury from a projectile or an object
So are you going to scan your children or not? There isn't an easy answer, and your approach is going to be influenced by the injury mechanism, the clinical situation, your intuition, the trust policy and the guidelines above. At the moment, even in children, we seem to err on the side of caution, and if in doubt, scan.
After you have scanned and discharged your children, or just discharged your children remember to give them some good quality head injury advice. The quality of advice leaflets is variable, and some of them make you look daft when they say return straight away if there is any vomiting - and you've sent them home with three discrete guy episodes! I find it useful to encourage brain rest (no computers!) and headway has some excellent advice. For serious injuries, the Child Brain Injury Trust has some excellent parent resources.
Parents often ask when their children can go back to sport. The brain is fragile and a second insult may be more damaging. Consider the use of the "SCAT3" (Sport Concussion Assessment Tool).
There's a case for you to consider here, and a different case to contemplate.
There's a case for you to consider here, and a different case to contemplate.
There's also a very useful case report here:
ReplyDeletehttp://adc.bmj.com/content/98/9/696.extract
It's a bit worrying too...
There's also an excellent review of vomiting from St Emlyns:
ReplyDeletehttp://stemlynsblog.org/2012/07/bumps-brains-and-barf/
It's nice to know that my sentiments are echoed!
http://dontforgetthebubbles.com/traumatic-brain-injury/ has got a good case report.
ReplyDeletehttp://www.medscape.com/viewarticle/813436?nlid=40783_545&src=wnl_edit_medp_emed&uac=187940MV&spon=45
ReplyDeletehttp://dontforgetthebubbles.com/head-injury-who-to-scan/#more-4582
ReplyDeleteNew guideline summary:
ReplyDeletehttp://stemlynsblog.org/updated-nice-head-injury-guidelines-worth-scan/
http://pedemmorsels.com/hypertonic-saline-tbi/
ReplyDeletehttp://www.ncbi.nlm.nih.gov/pubmed/24635987
ReplyDeletehttp://stemlynsblog.org/?p=6652
ReplyDeleteChris Partyka (@chrispartyka) tweeted at 0:30 AM on Fri, May 30, 2014:
ReplyDeletePECARN Paediatric CHI rule - #FellowshipFlashcards #FACEM https://t.co/ZEEM8Ccj9P
(https://twitter.com/chrispartyka/status/472157949108817920)
Get the official Twitter app at https://twitter.com/download
http://rolobotrambles.com/2014/06/20/what-i-learnt-this-week-accepting-im-a-curator-and-examiner-of-knowledge-rather-than-a-gatekeeper-of-it-wiltw/
ReplyDeleteAndrew Petrosoniak (@petrosoniak) tweeted at 8:04 PM on Sat, Jul 26, 2014:
ReplyDeleteOutstanding resource for management of peds concussions. Dx to Rx. A Must read http://t.co/2xYuItcGny #FOAMed #FOAMped @DocMaximum @eUSMD
(https://twitter.com/petrosoniak/status/493109635444781056)
Get the official Twitter app at https://twitter.com/download
http://www.aliem.com/vomiting-kids-head-trauma-ct/
ReplyDeletehttp://stemlynsblog.org/head-injury-in-children-decision-rules-pecarn-chalice/
ReplyDeleteNice post you're really helping the people about Head injury treatments and I also suggest this post Head Injury Treatment in Ludhiana
ReplyDelete